90/M ? TB MENINGITIS with ?PTB
case of 90 year old male came with complaints of
c/o cough since 15 days
SOB since 1 week
Loss of appetite since 1 week
Altered sensorium since 3 days



HOPI:
Patient was apparently asymptomatic 15 days ago then he developed cough insidious onset initially dry later productive and scanty.white to yellow not blood stained more during night. SOB since 1 week insidious onset gradually progessive ,progressed to grade 4, no orthopnea, No PND.No h/o seasonal/diurnal variation.
Loss of appetite since 1 week. No h/o fever, vomiting,pain abdomen,loose stools,giddiness. Altered sensorium since 3 days.
No relevant history in the past
Personal history:
Diet: mixed
Appetite: normal
Sleep: Adequate
Bowel and bladder: increased micturition(since 1week), normal bowel movements
No addictions and allergies
GENERAL EXAMINATION:
Vitals:
BP 120/70 MMHG
PR 92 BPM
RR 28/MIN
GRBS 93 MG/DL
SpO2 100% ON 6L O2
No pallor,No icterus, cyanosis, clubbing, lymphadenopathy.
SYSTEMIC EXAMINATION ::
GIT
INSPECTION :
Abdomen - scaphoid
Umbilicus - inverted
Movements - all quadrants are equally moving with respiration
No scars and sinuses
No visible peristalsis
No engorged veins.
PALPATION:
No local rise in temperature and no tenderness in all quadrants
LIVER: no hepatomegly
SPLEEN- not enlarged
KIDNEYS - bimanual palpable kidneys
PERCUSSION :
no shifting dullness
AUSCULTATION :
Bowel sounds are heard and are normal
No bruit
Respiratory system:
Inspection:
No tracheal deviation
Chest bilaterally symmetrical
Type of respiration: thoraco abdominal.
No dilated veins,pulsations,scars, sinuses.
No drooping of shoulder.
Palpation:
No tracheal deviation
Apex beat- 5th intercoastal space,medial to midclavicular line.
Tenderness over chestwall- absent.
Vocal fremitus- normal on both sides.
Percussion:
Supraclavicular
Infraclavicular.
Mammary
Axillary
Infraaxillary
Suprascapular
Infrascapular
Interscapular
Right side and left side- resonant in above areas.
Auscultation:
Bilateral Airway entry - present.
Decreased BS on the left side.
B/L crepts present in basal areas,wheeze present.
Cardiovascular system:
Inspection : no visible pulsation , no visible apex beat , no visible scars.
Palpation: all pulses felt , apex beat felt.
Percussion: heart borders normal.
Auscultation:
Mitral area, tricuspid area, pulmonary area, aortic area- S1,S2 heard.
Central Nervous system:
Higher motor functions- cannot be elicited
Speech: Normal
Cranial nerve functions - cannot be elicited
Sensory system- cannot be elicited
Motor system Right Left
Power- UL 4/5 4/5
LL 4/5 4/5
Neck Normal
Trunk muscles Normal
Tone- UL Normal Normal
LL Normal Normal
Reflexes-
Superficial reflexes - Intact
Plantar flexion flexion
Deep tendon reflexes -
Biceps + +
Triceps + +
Supinator + +
Knee + +
Ankle + +
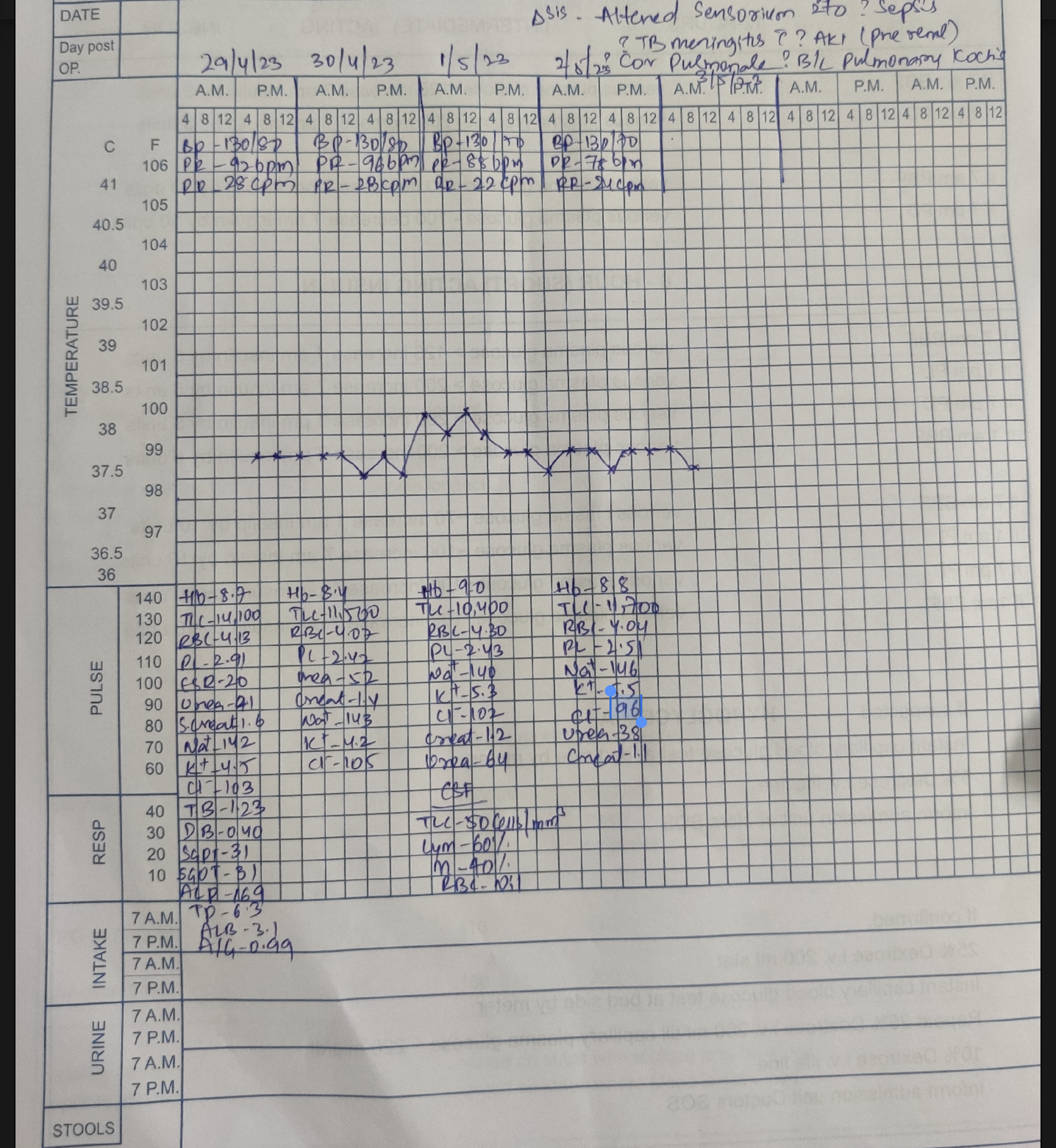
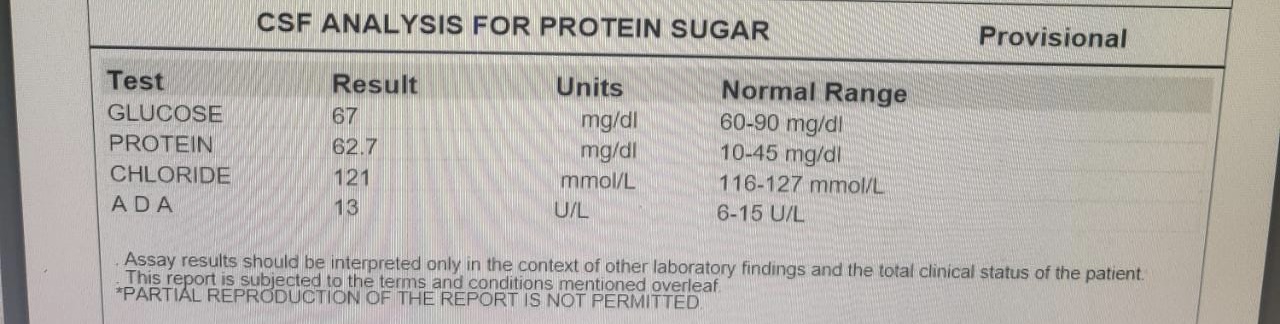
INVESTIGATIONS:
29/4/23









2/5/23





DIAGNOSIS :
Altered sensorium secondary to ? TB meningitis ? pyogenic meningitis
?AKI ( Pre renal) resolved
?COPD(emphysematous)
? B/L pulmonary koch's with iron deficiency Anemia
TREATMENT:
1. IV FLUIDS NS @ 75 ml/hr
2. RT feed
200 ml water 2 nd hrly
200 ml milk 4th hrly
3. Nebulization with budecort - 12 th hrly
Duolin -6 th hrly
Mucomist - 4 th hrly
4.SYP.GRILLINCTUS - 15 ml RT/TID
5.CPAP - Intermittently
6.Oxygen support to maintain spo2 88-94%
7.GRBS - 7 POINT PROFILE
8.Vitals monitoring 2nd hrly
Thanks to dr.tharun adn dr.deepthi interns posted in dept of general medicine for the daily soap notes and fever chart
30/4/23
S
Stools passed
No fever
O
Pt is conscious, coherent and irritable
Speech is normal
No meningeal signs
GCS E 4 V4 M5
BP - 130/80 mm hg
PR - 92 bpm
SPO2: 96% ON 6L O2
RR: 28 cpm
CVS: S1S2 + , NO MURMURS
RS: BAE+ , B/L CREPTS + ,WHEEZE +
CNS: E4V4M5
Rt lt
Tone UL N N
LL N N
Power UL 4/5 4/5
LL 4/5 4/5
Reflexes
R L
B + +
T + +
S + +
K + +
A + +
P + +
P/A: SOFT, NON TENDER
I/O:1800ml/800ml
GRBS: 108MG/DL
A
Altered sensorium secondary to ?sepsis ? TB meningitis
?AKI ( Pre renal)
?Cor pulmonale
? B/L pulmonary koch's with iron deficiency anemia
P
1. IV FLUIDS NS @ 75 ml/hr
2. RT feed
200 ml water 2 nd hrly
200 ml milk 4th hrly
3. Nebulization with budecort - 12 th hrly
Duolin -6 th hrly
Mucomist - 4 th hrly
4.SYP.GRILLINCTUS - 15 ml RT/TID
5.CPAP - Intermittently
6.Oxygen support to maintain spo2 88-94%
7.GRBS - 7 POINT PROFILE
8.Vitals monitoring 2nd hrly.
1/5/23
S
Stools passed
No fever
O
Pt is conscious, Not coherent to time,place, person and irritable
Speech is normal
No meningeal signs
GCS E 4 V4 M5
BP - 120/80 mm hg
PR - 84 bpm
SPO2: 92% ON RA
RR: 24 cpm
CVS: S1S2 + , NO MURMURS
RS: BAE+ ,WHEEZE(Expiratory) +
Rt lt
Tone UL N N
LL N N
Power UL 4/5 4/5
LL 4/5 4/5
Reflexes
R L
B + +
T + +
S + +
K + +
A + +
P + +
P/A: SOFT, NON TENDER
I/O:2400ml/1050ml
GRBS: 124MG/DL
A
Altered sensorium secondary to ? Pyogenic meningitis ? TB meningitis With AKI (pre renal) resolving
?Cor pulmonale with COPD( emphysematous)
? B/L pulmonary koch's with iron deficiency anemia
P
1. IV FLUIDS NS @ 75 ml/hr
2. RT feed
200 ml water 2 nd hrly
200 ml milk 4th hrly
3. Nebulization with budecort - 12 th hrly
Duolin -6 th hrly
Mucomist - 4 th hrly
4.SYP.GRILLINCTUS - 15 ml RT/TID
5.CPAP - Intermittently
6.Oxygen support to maintain spo2 88-94%
7.GRBS - 7 POINT PROFILE
8.Vitals monitoring 2nd hrly.
2/5/23
S
No fever spikes
O
Pt is conscious, Coherent to person, Not coherent to time,place and irritable
Speech is normal
No meningeal signs
GCS E 4 V4 M6
BP - 130/70 mm hg
PR - 74 bpm
SPO2: 91% ON RA
RR: 22 cpm
CVS: S1S2 + , NO MURMURS
RS: BAE+ , B/L WHEEZE + R>L
Rt lt
Tone UL N N
LL N N
Power UL 4/5 4/5
LL 4/5 4/5
Reflexes
R L
B + +
T + +
S + +
K + +
A + +
P + +
P/A: SOFT, NON TENDER
I/O:2400ml/1400ml
GRBS: 131MG/DL
A
Altered sensorium secondary to ? TB meningitis ? Pyogenic meningitis with AKI (pre renal) resolved with
? COPD( emphysematous)
? B/L pulmonary koch's with iron deficiency anemia
P
1. IV FLUIDS NS @ 75 ml/hr
2. RT feed
200 ml water 2 nd hrly
200 ml milk 4th hrly
3.Inj.MONOCEF 2g IV/BD
3. Inj.LASIX 40mg iv /OD 4.Nebulization with budecort - 12 th hrly
Duolin -6 th hrly
Mucomist - 4 th hrly
5.SYP.GRILINCTUS - 15 ml RT/TID
6.CPAP - Intermittently
7.Oxygen support to maintain spo2 88-92%
8.GRBS - 6th hrly.
9.Vitals monitoring 2nd hrly.
10.Tab.RIFAMPICIN 150mg
Tab.ISONIAZID 75MG
Tab.PYRIZINAMIDE 400MG
Tab.ETHAMBUTOL 275MG
11.Tab.PYRIDOXINE 50MG PO/OD
3/5/23
S
No fever spikes
O
Pt is conscious, Coherent to time and person, Not coherent to place and slightly irritable
GCS E 4 V5 M6
BP - 120/80 mm hg
PR - 92 bpm
SPO2: 91% ON RA
RR: 22 cpm
CVS: S1S2 + , NO MURMURS
RS: BAE+ , Rt. IAA,ICA,IMA Expiratory rhonchi present
Rt lt
Tone UL N N
LL N N
Power UL 4/5 4/5
LL 4/5 4/5
Reflexes
R L
B + +
T + +
S + +
K + +
A + +
P + +
P/A: SOFT, NON TENDER
I/O:2900ml/1750ml
GRBS: 112MG/DL
A
Altered sensorium secondary to ? TB meningitis ? Pyogenic meningitis with AKI (pre renal) resolved with
COPD( emphysematous)
B/L pulmonary koch's with iron deficiency anemia
P
1. IV FLUIDS NS @ 75 ml/hr
2. RT feed
200 ml water 2 nd hrly
200 ml milk 4th hrly
3.Inj.MONOCEF 2g IV/BD
4. Inj.LASIX 40mg iv /OD
5.Tab.RIFAMPICIN 150mg
Tab.ISONIAZID 75MG
Tab.PYRIZINAMIDE 400MG
Tab.ETHAMBUTOL 275MG
6.Nebulization with budecort - 12 th hrly
Duolin -6 th hrly
Mucomist - 4 th hrly
7.Oxygen support to maintain spo2 88-92%
8.GRBS - 6th hrly.
9.Tab.PYRIDOXINE 50MG PO/OD
10.Vitals monitoring 2nd hrly.
11.Chest physiotherapy

ATT started from 2/5/23



Comments
Post a Comment