55M MALNUTRITION ASCITIS ? TB PERITONITIS WITH LEFT PLEURAL EFFUSION
A 55 YEAR OLD MALE CAME WITH C/0
ABDOMINAL DISTENTION SINCE 1 MONTH
DECREASED APPETITE SINCE 20 DAYS
FEVER SINCE 10 DAYS
HOPI: 55YEAR OLD MALE RESIDENT OF NARKETPALLY MECHANIC BY OCCUPATION , CHRONIC ALCOHOLIC SINCE 30 YEARS 2 QUARTERS PER DAY AND CHRONIC SMOOKER SINCE 30 YEARS , 10 BEEDIS PER DAY HIS WIFE EXPIRED 3 YEARS AGO FROM THEN HE INCREASED THE ALCOHOL INTAKE .
PATIENT WAS APPARENTLY ASYMPTOMATIC 1 MONTH BACK, THEN DEVELOPED ABDOMINAL DISTENTION WHICH IS INSIDIOUS IN ONSET AND GRADUALLY PROGRESSIVE.
FEVER SINCE 10 DAYS WHICH IS OF HIGH GRADE, ASSOCIATED WITH CHILLS AND RIGORS, RAISED DURING EVENING AND NIGHT AND RELIEVED ON MEDICATION.
HE ALSO HAD DECREASED APPETITE SINCE 20 DAYS
H/O BLACK COLOURED STOOLS FROM 10 DAYS
NO H/O PAIN ABDOMEN
NO H/O VOMITING
NO H/O LOOSE MOTIONS/CONSTIPATION
NO H/O BURNING MICTURITION
NO H/O HEMOPTYSIS
PAST HISTORY:
N/K/C/O HTN/DM/TB/CAD/CVA/THYROID DISORDER/EPILEPSY
PERSONAL HISTORY:
DIET- MIXED
APPETITE- DECREASED
SLEEP- ADEQUATE
BOWEL AND BLADDER MOVEMENTS- REGULAR
ADDICTIONS-
HE IS A CHRONIC ALCOHOLIC SINCE 30 YEARS( 2 QUARTERS/DAY). STOPPED SINCE 20 DAYS.
HE IS ALSO A CHRONIC SMOKER SINCE 30 YEARS( 9 BEEDI/DAY)
ON EXAMINATION:
PATIENT IS CONSCIOUS, COHERENT, COOPERATIVE
PALLOR- ABSENT
ICTERUS- ABSENT
CYANOSIS- ABSENT
CLUBBING- ABSENT
LYMPHADENOPATHY- ABSENT
EDEMA- ABSENT
VITALS :
AT THE TIME OF ADMISSION :
TEMP. : 97.2
PR : 88 BPM
RR : 18 CPM
BP : 100/60 MM HG
SpO2 : 98%
GRBS:108 GM/DL
WEIGHT-49. 4KGS(6/7/23)
49KGS(7/3/23)
48. 6KGS(8/3/23)
47. 6KGS(9/3/23)
47. 58 KGS(10/3/23)
ABDOMINAL GIRTH-
77.8CMS(6/3/23)
77.5CMS(7/3/23)
77 CMS(8/3/23)
73CMS(9/3/23)
78. 5CMS(10/3/23)
ON SYSTEMIC EXAMINATION:
CVS : S1, S2 HEARD
RS : BAE PRESENT
DECREASED BREATH SOUNDS IN LEFT IAA
P/A : TENDERNESS PRESENT IN EPIGASTRIC AND UMBLICAL REGIONS



CNS : HMF INTACT
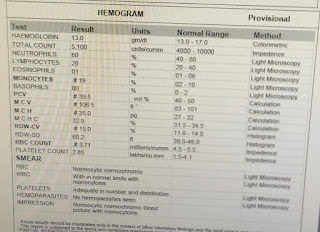
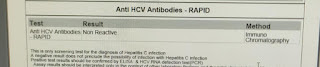
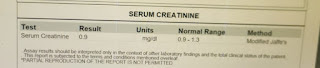
INVESTIGATIONS:
ON 28/2/23









ON 6/3/23













ON 7/3/23:



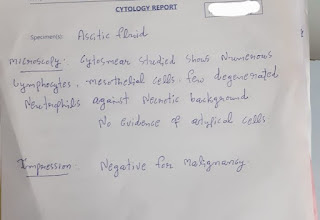

ASCITIC TAP IS DONE ON 6/3/23-
ASCITIC TAP OF 450ML WAS DONE

On 8/3/23:















ASCITIC TAP WAS FONE(8/3/23) -
ASCITIC TAP WAS DONEOF 150ML


X ray done post ascitic tap

LIGHT'S CRITERIA-

ASCITIC FLUID Add

On 9/3/34




10/3/23


MANTOUX TEST:DONE ON 8/3/23
BEFORE TEST

DAY 0

DAY1

DAY 2

DAY3

PROVISIONAL DIAGNOSIS:
ASCITIS UNDER EVALUATION(LOW SAAG HIGH PROTEIN ) SECONDARY TO
?CHRONIC LIVER DISEASE TO RULE OUT SPONTANEOUS BACTERIAL PERITONITIS
?TB PERITONITIS
LEFT PLUERAL EFFUSION
TREATMENT:
1) SALT RESTRICTION<2GM/DAY
2) FLUID RESTRICTION<1.2LIT/DAY
3) INJ CEFTOXIME 1GM IV/BD
4) INJ PAN 40MG IV/BD
5) INJ LACILACTONE20/25 PO/OD@9AM
6) SYP LACTULOSE 10ML PO/BD
7) TAB DOLO 650MG PO/TID
8) STRICT INPUT /OUTPUT CHARTING
Evidence to start ATT :
1)Ascitic & pleural cells=Lymphocytic predominant
2)Ascitic ADA=100(<30 normal)
3)Exudative pleural effusion
4)Low SAAG High protien
wats app conversation by Dr.KEERTHI MADIREDDI PGY2
India’s Revised National TB Control Programme guidelines which recommend that patients with two negative sputum smear results should be treated with broad-spectrum antibiotics for 2 weeks with a follow-up chest X-ray if symptoms persist.
but in this case ascitic and pleural fluid shows lymphocytic predominance , ascitic ada is pointing towards TB most likely so starting ATT empirically and keeping a regular followup with the patient will be helpful sir
on 10 th march gastroenterologist opinion taken
adviced
To start ATT now
To avoid pyrazinamide in ATT as the patient already has background CLD asked to speak with pulmonology dept for fixing dose
CT scan can be adviced to check for any malignancy.
on 11 th march pulmonology opinion taken

Patient diagnosed as TB PERITONITIS came for follow up on 20th march 2023 and is doing well |
Patient came for follow up on 8th april 2023 and has no complaints.
He is receiving ATT from Nalgonda district hospital


His LFT ON 8-4-2023
The patient was contacted via phone calls and communication was made with his daughter. He received ATT from the local government hospital and discontinued ATT after one year as instructed by the doctor at the government hospital. The patient is doing well and has no complaints.
OUTCOME - COMPLETELY RECOVERED

Comments
Post a Comment